
Table of Contents
- Definition
- Benign Prostatic Hyperplasia Types
- Symptomatology
- Who Is in the Risk Group?
- Why is Benign Prostatic Hyperplasia Dangerous?
- Does BPH Mean Surgery or Not?
- BPH Patient Examination
- Benign Prostatic Hyperplasia Treatment
» Benign prostatic hyperplasia is a pathologic benign growth of prostatic gland. It is important to recognize BPH and differentiate it from other pathologies. The most probable risk factors are age, production of male sex hormones, and genetic predisposition.
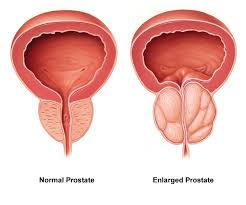
Benign Prostatic Hyperplasia (BPH): Definition
Benign prostatic hyperplasia (BPH) is a pathologic benign growth of prostatic gland. Nodules appear around urinary tract. Their growth is accompanied by gradual compression. Benign character of BPH means that the process does not metastasize which is the main difference of hyperplasia from prostate carcinoma. In order to recognize benign prostatic hyperplasia and differentiate it from other pathologies, men over 40-50 years of age should attend a urologist regularly and undergo preventive examination approximately once per year.
Benign Prostatic Hyperplasia Types
Neoplastic process involves glandular, muscular, and connective tissues. And the pathology character may be adenomatous, fibrous, and myomatous accordingly. Benign prostatic hyperplasia may differ in accordance with its form (spherical, bulb-shaped, cylinder-shaped), structure (composed of one or several nodules), and weight (in average from 5 to 200 grams).
There are three variants of BPH directions depending on its growth and location:
- Growth inside the urinary bladder. BPH penetrates into urinary bladder through urethra. This leads to deformation of inner constrictor and disturbs its function.
- Growth toward straight intestine. While expanding, BPH leads to insignificant disorder of urination. But this process is connected with urethra loss of its contractile force which prevents from complete bladder emptying.
- Uniform induration of prostatic gland. This is the most benign type of BPH. In this case, prostatic gland doesn’t increase, urinary retention and inappropriate urination are not observed.
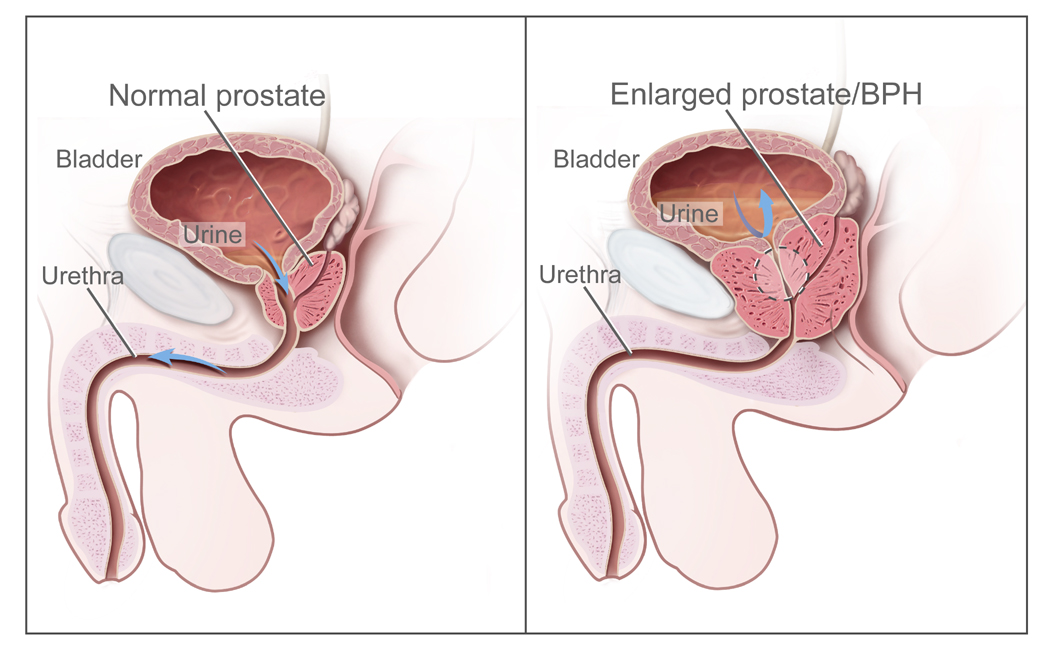
Symptomatology
Prostatic hyperplasia leads to growth of organ and narrowing of urethra with age. The degree of inappropriate urination depends to a greater extent not on the size of BPH, but on direction of its growth. Thus, hyperplasia of small size growing from back gland and hanging over urethra is capable to cause urinary retention, whereas considerable hyperplasia growing near collateral external glands of prostate toward straight intestine may not declare itself clinically.
- Frequent or difficult urination. In connection with peculiarities of urinary bladder functions, urination becomes more frequent at night time by up to 3-4 times. In the afternoon, a man may not notice or ignore the disease symptoms. Very often weakening of urine stream and difficult urination stay unnoticed being one of the first symptoms of benign prostatic hyperplasia at the same time.
- Feeling of incomplete emptying. It is sometimes confused with frequent urination which is observed in the morning. In this case a patient suffering from BPH has to urinate 3-4 times every 10-15 minutes. In the afternoon, the urination frequency is normal.
- Imperative desire to urinate. Sudden hardly restrained urges may occur any moment. This symptom demonstrates the progressive state of BPH.
- The afore-mentioned symptoms build up gradually. Very often a man attributes these conditions to age, stressful situations, and other factors. But the intensity of symptomatology and diagnostics of BPH differs considerably both in various age groups and the same age category.
For instance, around 40% of patients with exposed BPH complain of inappropriate urination, whereas only 20% of them seek medical attendance.
Who Is in the Risk Group?
Benign prostatic hyperplasia is characteristic to aged man. Detailed examination reveals the signs of the disease among 25% of patients at the age of 40-50 years, among 50% - of 50-60 years, among 80% - of 70-80 years, more than 90% of patients over 80 years.
Exact causes of hyperplasia appearance have not been revealed yet. The most probable risk factors considered by medical experts are age, production of male sex hormones, and genetic predisposition as well. It is proved that asexualized men either before or after sexual maturity are not prone to benign prostatic hyperplasia. Influence of alcohol, smoking, overweight, and sexual activity haven’t found scientific support.
Why is Benign Prostatic Hyperplasia Dangerous?
Hyperplasia of prostatic gland requires constant control. It is distinguished by augmenting of symptoms with the course of time and development of complications. In case the BPH therapy measures are not taken, prostatic gland will continue its growth resulting not only in difficult urination, but also in other more dangerous consequences. In order to avoid diverse complications of benign prostatic hyperplasia, it is required to seek immediate medical attendance.
Urinary tract infections.
They include cystitis, prostatitis, pyelonephritis. These diseases often accompany BPH. They are connected with development of breeding grounds for bacterial growth which occurs because of urine stagnation in bladder. Occurred inflammations aggravate the situation exacerbating considerably the quality of life. BPH accompanied by inflammation is characterized by lower back pain, as well as burning with urination, incontinence, frequent urination, bad smell of urine, and other symptoms. A large number of leucocytes attesting the inflammatory process occurrence are found after common urine analysis.
Acute urinary retention.
This frequent complication of BPH occurring after alcohol and some pharmaceutical drugs intake. The cause of this may be undergone abdominal operation or stressful situation. In this case, prostatic gland becomes swollen resulting in impossibility of urination due to complete overlapping of urethra. Urinary bladder becomes overfilled, and a patient cannot void it without assistance. Principal symptoms – strong urge to urinate, pain and pronounced discomfort below waist. This situation requires immediate medical intervention.
Hydronephrosis.
In case of hydronephrosis, urine is not cleared, but overfills kidney. This is a dangerous condition caused by benign prostatic hyperplasia and accompanied by lower back pain, strong urge for urination, and impossibility to empty the bladder. Other symptoms may be represented by high temperature, nausea, and vomit. This condition generally develops with acute urinary detention and may cause a chronic renal insufficiency. Hydronephrosis requires immediate medical intervention.
Lithiasis.
This is a frequently-met complication of BPH. Occasionally found bladder stones may be the only symptom of the disease. Their development may be caused by long-term urine accumulation. The key symptoms of stones presence may be urination pain, blood in urine, frequent urination or acute urination detention.
BPH death rate.
According to research studies, mortality cases with BPH are connected with complications development occurred as a result of prompt treatment absence. Three main causes of death may be chronic renal insufficiency, incidence (sepsis) and complications after surgery.
Does Benign Prostatic Hyperplasia Mean Surgery or Not?
There is no necessity to intervene with vital processes of organism. Along with indications there are counter-indications to any method of treatment. Therefore, the final decision rests with doctors of practicability and efficiency pf surgery which may be based on the principle of adequate care. Moreover, lately reference is made to gradual reduction of number of patients who are prescribed surgical treatment. This phenomenon is connected with prompt diagnostics allowing administering conservative therapy which decreases necessity of surgery.
Benign Prostatic Hyperplasia Patient Examination
Therapeutic approach for a patient suffering from benign prostatic hyperplasia must be determined after preliminary examination.
In accordance with World Health Organization, minimal list of examinations includes:
- filling out a special questionnaire IPSS containing seven questions;
- estimation of life quality according to 6-point scale (QQL);
- digital rectal examination;
- common urine examination;
- BUN and creatinin content in serum;
- ultrasound investigation of prostatic gland to determine presence and quantity of residual urine;
- uroflow speed study;
- prostate detection of prostate-specific antigen in serum (increase of PSA level may signalize prostate carcinoma);
- if necessary, kidney roentgen-ray survey;
- urination diary (registration of urinations and volume of urine during 2-3 days);
- in case of increased level of PSA or suspected prostatic affection after digital rectal examination, prostate biopsy is required.
Treatment of Benign Prostatic Hyperplasia

Possible variants of treatment are surgical intervention, drug therapy and case monitoring.
Case Monitoring
Based on the modern assumption, the drug therapy must be prescribed for BPH patients with initial manifestations of inappropriate urination without involvement in the process of upper urinary tract and complications, patients with relative and absolute counter-indications to operative treatment, and patients delaying it for various reasons. According to statistics, these patients make 60-70% of all patients suffering from diverse urination difficulties due to benign prostatic hyperplasia. Case monitoring is admissible for patients with mild symptomatology the whose life quality is not affected significantly because of the existing symptoms and implies control over urine and blood examination, PSA, ultrasound investigation and uroflow every 6-12 months. This strategy implies implementation of elements of behavior therapy: fluid restriction in the evening, food with diuretic action rejection (fruits, tea, coffee, alcohol), correction of concomitant drug therapy, etc.
Surgical intervention
Surgical intervention is indicative to patients with pronounced symptomatology, involving in the process of upper urinary tract and those who have counter-indications to drug therapy or the latter doesn’t give desired effects. The aim of each operation is removal of hyperplastic tissue of prostatic gland which narrows lumen of urinary tract preventing from normal urination. I.e. the prostatic gland is not removed completely, but only a part of it which oppresses urethra. There are three types of surgeries:
- subcutaneous operation. This is a transurethral prostatic resection which is in fact a golden standard of BPH surgical treatment. Operation is performed without incision; the instrument is introduced through urinary tract.
- laser ablation or enucleation of prostatic gland. This is a subcutaneous operation in the course of which laser but not electric energy is used in comparison with transurethral prostatic resection. Bleeding during the operation is lower, but radicalism while ablation yields to transurethral prostatic resection. Laser enucleation is used in case of considerable expansion of prostatic gland and is an alternative of an open operation.
- open operation – adenomectomy. This operation is performed in case of pronounced growth of prostatic gland when transurethral resection of the prostate is technically impossible. An incision of 6-10 cm is performed above pubic articulation along abdominal midline.
- minimally invasive operations (transurethral needle ablation of the prostate, microwave thermotherapy, etc.) may be conducted for aged patients with a large quantity of background diseases. All these operations have less efficiency in comparison with transurethral prostatic resection and adenomectomy, but their risk is also much lower.
Subject to your general state, accompanying diseases, degree of prostate growth (volume), complications and other factors, your attending doctor will recommend you the proper surgery type.
Drug therapy
 Operative intervention has the highest efficiency rate, and at the same time – the highest percentage of complications and not always will release a patient from all symptoms of urination disorders. For the last 10-15 years there is a steady tendency to reduction of popularity of operative methods of benign prostatic hyperplasia treatment. Drug therapy is conducted among 70% of patients. Success of modern pharmacology provided a big variety of medicines for BPH. Their selection is mainly explained by degree of manifestation of some or other symptoms, peculiarities of the disease, and physical examination data. With all variety of drug therapy of benign prostatic hyperplasia, urologists from all over the world have formulated the main principles of its conducting based on the degree of proof, efficiency and safety of medicines.
Operative intervention has the highest efficiency rate, and at the same time – the highest percentage of complications and not always will release a patient from all symptoms of urination disorders. For the last 10-15 years there is a steady tendency to reduction of popularity of operative methods of benign prostatic hyperplasia treatment. Drug therapy is conducted among 70% of patients. Success of modern pharmacology provided a big variety of medicines for BPH. Their selection is mainly explained by degree of manifestation of some or other symptoms, peculiarities of the disease, and physical examination data. With all variety of drug therapy of benign prostatic hyperplasia, urologists from all over the world have formulated the main principles of its conducting based on the degree of proof, efficiency and safety of medicines.
- The most popular medicines are alpha-adrenergic blocking agents. They provide a perfect result occurring right after the beginning of therapy due to their effectiveness and well tolerability. The duration of the treatment course is from several months to several years. In majority of cases, therapy is designed for constant intake of medicines. But alpha-adrenergic blocking agents do not prevent from prostatic gland growth.
- Inhibitors of 5-CoA reductase take their action in 6-12 months after constant administration and also imply long-term (years long) therapy course. Prescription of them by short courses is not effective. On the top of their administration it is possible not only stop prostatic gland growth but also achieve its reduction by 20-30%. The most popular scheme of inhibitors of 5-CoA reductase prescription is their combined intake with alpha-adrenergic blocking agents. Simultaneous intake of both drugs takes the biggest effect.
- M-anti-cholinergics (anticholinergic agents) are indicative to patients suffering from the so-called neurogenic urinary discomfort. They are also accompanied by prostate growth and united with the notion “hyperactive bladder”. This diagnosis shows the symptoms of accumulatory phase. The medications of this pharmacological group may be prescribed for independent use and in combination with other medicines.
- Plant-based medicines containing extracts of various plants are not recommended for patients suffering from benign prostatic hyperplasia due to their low efficiency and shortage of information proving the justifiability of such assignments.
The list of medicines which may be used for drug therapy is not confined to the afore-mentioned ones. For instance, in combination of urination discomfort symptoms with erectile dysfunction, PDE5 inhibitors are successfully applied, whereas patients suffering from pronounced nocturia (frequent urination at night) use the analogues of beta hypophamine.
» Urologists do not use clichéd treatment regimens of BPH and approach to the treatment of each patient individually. This allows achieving steady positive effect with minimal risk of complications and side-effects. It should be noted that the selected strategy either operative treatment, case monitoring or drug therapy requires regular examinations and specialist consultations for probably correction of conducted treatment.